
Acute Lymphoblastic Leukaemia (ALL) is a kind of blood cancer that grows quickly and needs to be treated right away. “Acute” signifies that it becomes worse quickly, as opposed to chronic leukaemias, which get worse slowly over time. Lymphoblastic implies it affects a certain type of white blood cell called lymphocytes, which are very important for your immune system.
Your bone marrow is like a factory that generates blood cells. In ALL, this factory starts making bad cells, which are immature white blood cells known as lymphoblasts (blast cells). These blast cells:
- don’t work right,
- too rapidly to multiply,
- and fill the space that healthy blood cells should be in.
The body starts to have difficulties including infections, fatigue, bleeding, and bruises as healthy cells die off.
This handbook explains everything in clear English. If you
Understanding Normal Blood Cell Production
Before we go deeper, let’s understand how healthy blood cell production normally works.
Your bone marrow (soft tissue inside bones) produces three main types of blood cells:
1) Red Blood Cells (RBCs)
RBCs carry oxygen from the lungs to all parts of the body. They help you stay active and energetic.
If RBCs become low, you may feel tired and weak. This is called anemia.
2) White Blood Cells (WBCs)
WBCs protect the body from infections (bacteria, viruses, and other germs).
There are different types of WBCs, and in ALL, the problem mainly affects lymphocytes.
3) Platelets
Platelets help blood clot after injury. They stop bleeding.
Low platelets can cause easy bruising, nosebleeds, or gum bleeding.
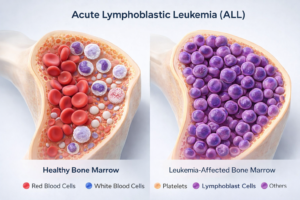
In a healthy body, the bone marrow keeps all these cells in balance.
What Happens in Acute Lymphoblastic Leukemia?
In ALL, the bone marrow starts producing large numbers of immature lymphocytes, known as lymphoblasts. These cells create two big problems:
Problem 1: They don’t mature
They stay “stuck” in an immature stage and cannot fight infections like normal WBCs.
Problem 2: They multiply without control
These cells keep dividing and fill the bone marrow and blood.
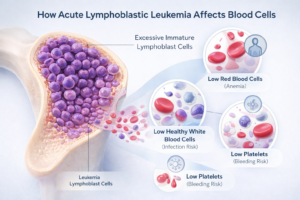
As the abnormal cells increase, they push out the healthy cells, which leads to:
Low red blood cells → anemia, weakness, paleness
Low healthy white blood cells → frequent infections, fever
Low platelets → bruising and bleeding
These leukemia cells can also travel to other parts of the body like:
lymph nodes
liver and spleen
brain and spinal cord
That’s why some patients develop swelling, belly fullness, headaches, or neurological symptoms.
Types of Acute Lymphoblastic Leukemia
ALL is not exactly the same in every patient. Doctors classify it mainly based on which type of lymphocyte is affected.
1) B-Cell ALL (B-Lymphoblastic Leukemia)
Most common type (about 75–80% cases)
More common in children
Often responds well to treatment
2) T-Cell ALL (T-Lymphoblastic Leukemia)
Less common (about 15–20% cases)
Often more aggressive
Seen more in teenagers and young adults
Doctors may also classify ALL based on genetic changes in leukemia cells, because this can affect treatment choice and prognosis.
Symptoms of Acute Lymphoblastic Leukemia
Symptoms usually start within weeks and may worsen quickly. Most symptoms happen due to low normal blood cells and build-up of leukemia cells.
A) Symptoms due to low red blood cells (Anemia)
constant tiredness
weakness
pale skin
shortness of breath during activity
dizziness
cold hands/feet
B) Symptoms due to low healthy white blood cells
frequent infections
fever (repeated or persistent)
infections that take long to improve
pneumonia or serious infections in some cases
C) Symptoms due to low platelets
bruising from small bumps
tiny red spots on skin (petechiae)
nosebleeds
gum bleeding
heavy periods in women
bleeding that takes time to stop
D) Symptoms due to leukemia cell build-up
Bone and joint pain:
Leukemia cells in bone marrow can cause pressure and pain. Children may complain of leg pain or limp, and sometimes refuse to walk.
Swollen lymph nodes:
Small lumps in neck, armpit, or groin.
Enlarged liver/spleen:
Feeling of heaviness or fullness in the belly.
Other symptoms:
poor appetite
weight loss
headache, vomiting, vision changes (if CNS involvement)
chest discomfort or breathing issues (sometimes with T-cell ALL)
Important Note for Children
In children, ALL may look like a normal infection initially. The key difference is:
symptoms don’t settle, and often become worse over 10–14 days.
Causes and Risk Factors
Many people ask: “Why did this happen?”
In most cases, doctors cannot find one exact cause. ALL happens due to DNA changes in developing lymphocytes, but what triggers these changes is often unknown.
Known risk factors
Genetic conditions (Down syndrome, Bloom syndrome, etc.)
High radiation exposure (rare situations)
Past chemotherapy/radiation for another cancer
Long-term exposure to some chemicals like benzene (industrial exposure)
What does NOT cause ALL
It’s not due to stress or emotions
It’s not contagious
It’s not caused by something a mother did in pregnancy (most cases)
No strong proof that normal daily electronics/power lines cause ALL
How Acute Lymphoblastic Leukemia is Diagnosed
Doctors do several tests to confirm ALL and plan treatment properly.
1) Blood tests
CBC (Complete Blood Count): checks RBC, WBC, and platelets
In ALL, RBC and platelets are often low. WBC may be high/low/normal.
Peripheral blood smear: blood is seen under microscope to look for blasts.
2) Bone marrow aspiration and biopsy
This is the main confirmatory test.
A sample is taken from pelvic bone. If blast cells are high (often >20%), ALL is diagnosed.
3) Flow cytometry (Immunophenotyping)
This tells whether it is B-cell ALL or T-cell ALL.
4) Cytogenetic & molecular tests
These check chromosome/gene changes that can guide treatment decisions.
5) Lumbar puncture (Spinal tap)
Doctors check if leukemia cells have reached the brain/spinal fluid.
Sometimes chemotherapy is also given through this route as prevention/treatment.
Risk Classification (Instead of Staging)
ALL doesn’t use “stage 1–4” like many cancers. Doctors use risk groups to decide treatment intensity.
Standard (Low) risk
age 1–9 years (especially children)
lower WBC count
good genetic features
quick response to early treatment
High risk
age 10 years or older
high WBC count
certain genetic changes
slower early response
Very high risk
very unfavorable genetics
poor early response
disease detected after initial treatment phase
infants under 1 year (in some cases)
Treatment of ALL in India (Phases + Options)
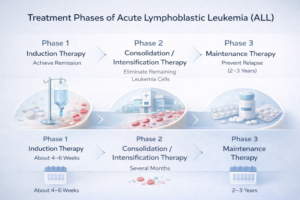
ALL treatment usually lasts 2–3 years, and is done in phases.
Phase 1: Induction
Goal: bring leukemia into remission
Duration: about 4–6 weeks
This phase is usually intensive and may require hospital stay due to infection risk.
Phase 2: Consolidation / Intensification
Goal: kill hidden leukemia cells
Duration: several months
Different drug combinations are used.
Phase 3: Maintenance
Goal: prevent relapse
Duration: 2–3 years
Often involves tablets + periodic hospital visits.
CNS protection (throughout treatment)
Because leukemia can affect brain/spinal cord, doctors give intrathecal chemo (medicine in spinal fluid) during treatment.
Treatment Options in Detail
1) Chemotherapy (Main treatment)
Chemo is the base of ALL treatment. Different medicines are used in combinations depending on risk group.
2) Targeted therapy
If a patient has certain genetic changes (example: Philadelphia chromosome), targeted drugs may be added as advised by oncologist.
3) Immunotherapy
Some medicines help the immune system identify and attack leukemia cells. These may be used in specific situations.
4) CAR T-cell therapy
A newer advanced option used mainly in relapsed/refractory cases (availability and cost may differ across India).
5) Bone marrow / stem cell transplant
Recommended mainly for:
high-risk disease in some cases
relapse cases
poor response to standard therapy
This is intensive and requires close monitoring and strong supportive care.
Cost of ALL Treatment in India
Costs vary based on hospital type, city, complications, and treatment plan.
Approximate ranges
Government hospitals: ₹1.5 lakh to ₹5 lakh
Private hospitals: ₹5 lakh to ₹15 lakh
Bone marrow transplant: ₹15 lakh to ₹25 lakh+
Extra costs may include:
travel and accommodation
infection management
supportive medicines
long-term follow-ups
Many hospitals and NGOs provide support options, so families can ask about financial assistance programs.
Side Effects of Treatment
Most side effects are temporary and manageable with medical support.
Common short-term side effects
hair loss
nausea/vomiting
mouth ulcers
fatigue
infection risk
bleeding/bruising
anemia (sometimes transfusions needed)
Possible long-term effects (varies)
fertility issues (some patients)
bone health changes
heart effects (with some drugs)
learning difficulties in some children (especially if CNS treatment needed)
Doctors monitor and manage side effects during and after treatment.
Survival Rate and Prognosis
Survival has improved a lot over the years.
General survival (approx.)
Children: 80–90% long-term survival
Standard-risk children: can be 90%+
Adults: around 35–60% (better in younger adults)
Prognosis depends on:
age
WBC count at diagnosis
genetic changes
how quickly remission occurs
overall health
Doctors often consider a patient “cured” if they remain in remission for 5 years after finishing treatment (most relapses happen earlier).
Living With ALL (Practical Guidance)
During active treatment
frequent hospital visits
possible admissions during intense cycles
infection precautions (hand hygiene, avoiding crowds when counts are low)
regular blood tests
Nutrition basics
balanced home food as tolerated
plenty of fluids
follow hospital food safety guidelines (especially when immunity is low)
Emotional support
It’s normal to feel fear, stress, anger, sadness, or confusion. Support can help:
counselling
patient groups
support from family/friends
talking openly with the doctor team
When to See a Doctor
Please consult a doctor if you or your child has:
fever for more than 10–14 days
repeated infections
unexplained bruising/bleeding
persistent tiredness and weakness
bone pain that doesn’t improve
swollen lymph nodes that don’t reduce
Many of these symptoms can happen due to other conditions too — but it’s best to get checked early.
Frequently Asked Questions (FAQ)
1. Is Acute Lymphoblastic Leukemia curable?
Yes, many patients — especially children — can be cured with timely treatment.
2. How fast does ALL progress?
ALL can worsen over weeks, so early diagnosis is important.
3. What is the difference between ALL and AML?
ALL affects lymphocytes; AML affects myeloid cells. Treatments differ.
4. Is ALL hereditary?
Most cases are not inherited. Risk is slightly higher in some genetic conditions.
5. Is leukemia contagious?
No. It does not spread from one person to another.
6. Is bone marrow transplant required for everyone?
No. It is mainly for high-risk or relapse cases.
7. Can adults survive ALL?
Yes. Survival is improving, especially in younger adults with modern treatment.
8. How long does treatment take?
Usually 2–3 years, with intensive early months and longer maintenance.
9. Can patients work during treatment?
Most people need rest during intensive treatment. Some may work limited hours during maintenance, depending on health.
10. What is the approximate cost in India?
It varies widely; government hospitals are cheaper, private hospitals cost more, and transplant is most expensive.
Medical Disclaimer
This article is for educational purposes only and does not replace medical advice. Diagnosis and treatment decisions should always be made with a qualified doctor or cancer specialist. If you notice symptoms of leukemia, seek medical care promptly.
Conclusion
Acute Lymphoblastic Leukemia (ALL) is a serious condition, but it is also one of the most treatable blood cancers, especially in children. The treatment journey can be long and emotionally challenging, but with early diagnosis, the right treatment plan, and supportive care, many patients recover and go back to normal life.
If symptoms feel unusual or don’t improve over time, don’t ignore them — early testing can save lives.